The NY Times reports a growing concern that women may be overusing statins, the go-to class of medications for lowering the bad type of cholesterol (LDL). Although there were early concerns about whether statins did more harm than good, the current data are pretty darn convincing that the medications are quite effective in managing cholesterol, and clearly reduce the chance of heart attack and stroke in those at increased risk of those outcomes.
So what gives? It all comes down to whether the benefits of the medications outweigh the risks. For the most part, the risks of these medications are fixed (although there is some suggestion that these risks are greater for men than for women). But the benefits depend on what epidemiologists call the baseline risk. That’s the chance, for example, that you will have a heart attack in the next year if you’re not treated.
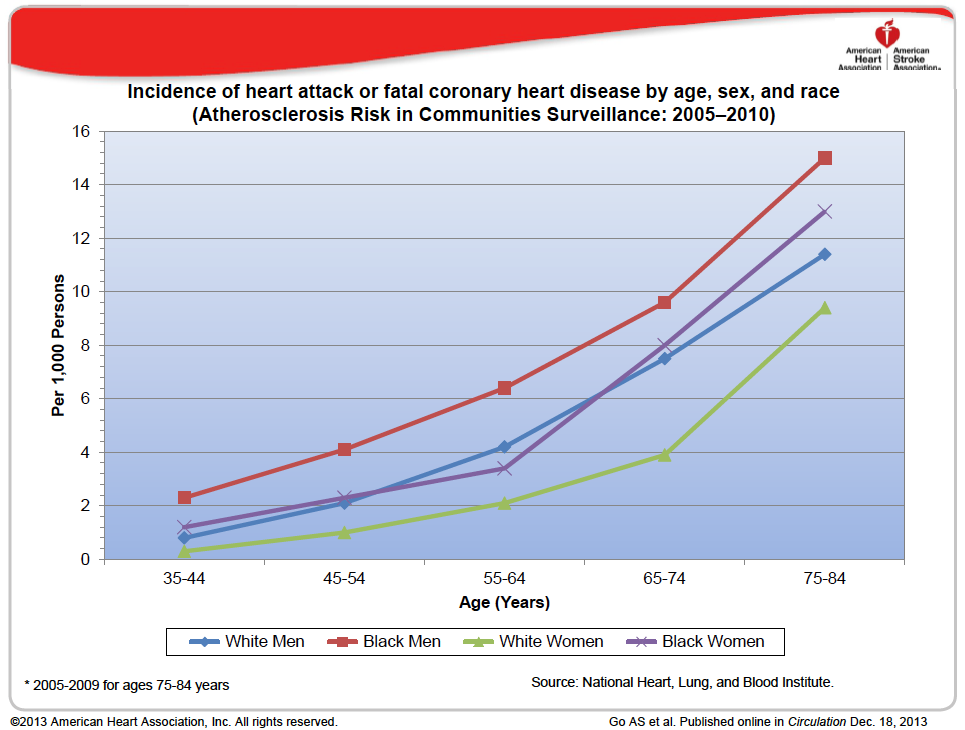
Although the risks of treatment are pretty much fixed, the baseline risk is not. It depends on your age, your sex, and your race… along with a host of other things such as your cholesterol levels, your family history, and whether you have diabetes.
To see why all of this matters, let’s assume that using statins cuts your baseline risk by half (they’re actually not quite that effective, but it makes the math easier). If your baseline risk is 10%, it gets cut to 5% — a reduction in the absolute risk of 5%. But if your baseline risk is 2%, it only gets cut to 1% — an absolute reduction of 1%.
All this means that whether the benefits of statins outweigh the risks depends not just on your cholesterol levels before you start treatment, but also your age, sex, race, and the like.
Take another look at the graph above. Roughly speaking, women’s risk at age X is about the same as men’s risk at age X – 10. That is, everything else being equal, you’d start a woman 10 years later than a man (except over about age 70, when women start catching up with men in terms of their risk).
The Fifty Bits Explanation of Why this is Happening
The rational approach to making decisions about the use of statins requires calculating the baseline risk in each individual patient. This takes work – not a lot of work, as there are plenty of calculators that will do the trick – but work nonetheless. Given our wiring for inattention and inertia, it’s a lot easier to just use a simple rule of thumb based on cholesterol levels.
In addition, it may be uncomfortable for a physician to treat two patients differently based on their sex or ethnicity. The facts are pretty solid but the social norms make it a bit of an uphill battle. And, as noted in the NY Times piece, quality indicators used to rank doctors and health plans don’t account for differences in patient mix, which may goose physicians to be more aggressive than they should otherwise be. And finally, the majority of physicians are supportive of the use of statins in patients with elevated cholesterol — regardless of the baseline risk. The urge to fit in may be counterproductive in this case.